The other day we had a patient with the most profound subcutaneous emphysema any of us had ever seen. The patient stated he’d just stumbled and hit the edge of a chair with his chest wall several days prior to presentation, then noticed he was “slowly getting bigger”. The family at the bedside all agreed that he was much bigger than usual.
On physical exam, he had normal vital signs, was in no distress, but had ‘the SQ crackles’ (crepitance) everywhere, and that’s not an exaggeration. Crepitance due to subcutaneous emphysema feels like popping tiny packing bubbles when compressed, and is usually limited to a fairly small area unless the patient is on the ventillator or getting positive pressures in the airway for some other reason.
Our patient got a CT to find where the air was coming from, and if there were other injuries. Here’s 3 slices from his CT:
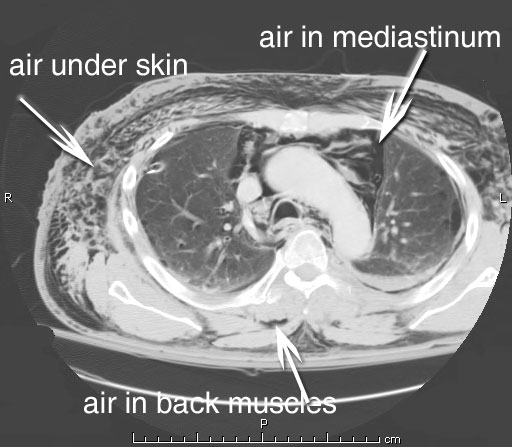
So, in the upper chest he has a respectable amount of SQ air, a pneumomediastinum, and air in other places.
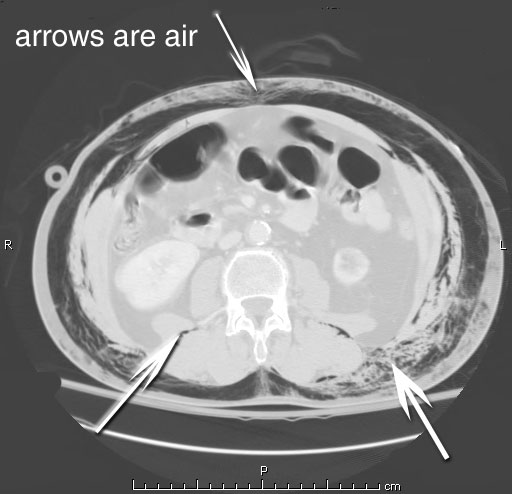
In the mid-abdomen the air continues, as well as being found in the back muscles.
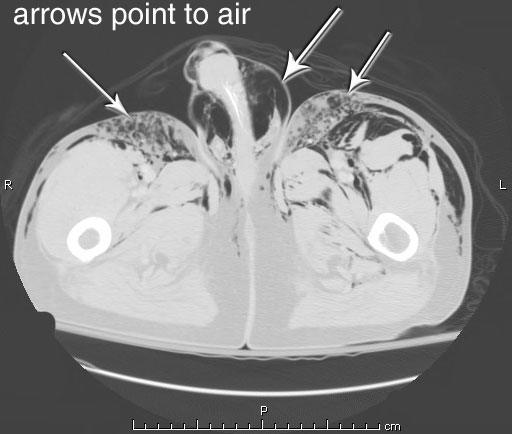
Here’s the part we didn’t expect: air in the skin of the penis, along with more SQ air.
He had crepitance literally everywhere, down to the tops of his feet. He got a right-sided chest tube for a pneumothorax that was felt to be the cause, and went upstairs.




Howdy Grunt Doc,
Wow, I’m an EMT student right now and we just learned about SE this week. Talk about timing…
Let me see if I read this correctly: The patient was slowly inflating himself, due to the pneumothorax?
You said that SE is usually associated with Pos. pressures. How much pressure are we talking? Are there any mechanisms other than pressure that are, usually, associated with SE?
Is it abnormal that the patient was feeling “normal” and had normal vitals? I would think, and I’m no expert, that a patient with pneumothorax would not “feel” very well.
I really like your site and you have been booked marked!
Take care,
Martinez
I didn’t say he felt normal, I said he was in no distress, there’s a difference.
This is a truly unusual case, which is why it is documented here. Most people with any SQ emphysema present very early, as they feel awful, and usually have abnormal vital signs.
Hypothesis alert! The only explanation I have for this is the following possible, very rare, set of circumstances: a patient with a 1-way valve from the inside of a lung to the outside (into the pleural space), and a second communication out into the subcutaneous space for the air, under the pressure of respiration to escape into. The ‘optimal injury’ for this would be a rib fracture which pokes a tiny hole in the lung and pleura at the same time, and which makes a communication into the SQ sapce as an added bonus. This would set up a ‘respiratory pump’ to push inspired air from the lung into the pleural space, the out into the SQ tissues, resulting in a slowly inflating patient.
Interesting.
Gives a whole new definition to the Austin Powers-esque penis-enlarging pump…
Was the patient Swedish?
You do see the most interesting cases! It’s hard to believe he got that much SQ air without being in more distress.
Hmmm…
Interesting to say the least. Was he by any chance a COPD’er?
I’ve seen SQ in the field, but nothing that extensive.
Great Blog, by the way.
Bill
Judy: not Swedish.
Thanks, Bill. Not a COPDer, no blebs elsewhere in the chest CT.
Okay, Grunt my-middle-name-is-Paul-Harvey Doc. Is there going to be “The rest of the story” on this? it’s just too weird
I have to say that I don’t necessarily agree with all the discussion on this case. Usually sub-q emphysema doesn’t occur from air “leaking” from the surface of the lung. It is due to air tracking back up a bronchovascular sheath, into the mediastinum, then fracturing the medistinal pleura and tracking into the sub-cutaneous fascia. This patient probably had some trauma to an airway, maybe even too small to be seen with a bronchoscope, and the air is tracking back toward the pleural reflection in the hilum. If the sub-q air didn’t resolve spontaneously, I’d do an airway exam.
Thanks for the input, Doug.
“Thanks for the input”
heh
That’s the first phrase they teach in Senior NCO academies….
“heh…That’s the first phrase they teach in Senior NCO academies…. ”
As in thanks for the input, now bugger off?
Aah, I knew I’d heard it before…
I saw a case of this when i was a student. I believe the patient’s methampehtamine lab had blown up on him.