CDC: If you subsidize something, you get more of it:
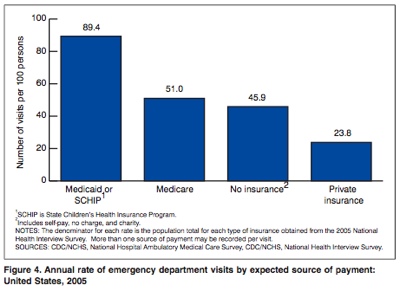
89% of Medicaid / Chip patients visited the ED; 51% of Medicare patients, etc. Hmm.
CDC: If you subsidize something, you get more of it:
89% of Medicaid / Chip patients visited the ED; 51% of Medicare patients, etc. Hmm.
Comments are closed.

Why not go to the ER? It’s free, right? Might as well have little Carlos checked out too. He was coughing just last week. And little Maria might have been exposed to strep throat at school.
I hate Medicaid “family plans.”
Come on…there are multiple factors at play here apart from “subsidies” and you know it. Persons with private insurance are younger, healthier and are less likely to go to the ER for this reason alone. Medicare and Medicaid patients are older, sicker and more likely to have chronic medical and mental illness. Of course they are more likely to end up in the ER.
I’ve had two patients go to the ER this week: A 77 year old woman with both Medicare and Medicaid and a h/o HTN, TIA’s and CRF who had N/V, Abd pain & inability to take p.o. She ended up having pancreatitis. The other was an 80 year old man–also on Medicare and Medicaid–a Russian immigrant with CAD s/p CABGx3, CHF with LVEF of
The only factor I care about is the one demonstrated here: a whole lot of people covered by government “free healthcare” show up in the ED. 89% of those covered, in fact. To the ED, despite the promise that ‘if they had coverage, they’ll be going to regular doctors to get their healthcare’, and that’s clearly not what’s happening.
I’m not buying the ‘private insurance are younger and healthier’ line, either. I see plenty of patients with multiple medical problems that have private insurance. Interesting that population shows up in ED’s less, though. Perhaps there is a realization it’s not ‘free’.
Where do you propose they go? If there are no general practitioners that accept Medicaid/CHIP, then where do they go? Cutting off the poor is one thing, but there needs to be some kind of public health system in their community prior to cutting them off.
And your argument would be better served if the Medicaid crowd were divided by their respective age/ethnicity etc.
Commenter 1 seems to imply that these Medicaid folks are immigrants. If that’s so, wouldn’t they be in the “no insurance” column?
Alrighty then . . . let’s roll up our sleeves here a bit, dr. grunt.
Assuming this measure is actually an appropriate one to support your rather sweeping macroeconomic conclusion (confounds be damned), please explain this:
Increase in visit rate (number of visits per 100 persons) – 2004-2005:
Private insurance
2004: 20.3
2005: 23.8
Increase: 17.24%
Medicaid/SCHIP
2004: 80.3
2005: 89.4
Increase: 11.33%
http://www.cdc.gov/nchs/data/ad/ad372.pdf
Ah . . . stats. What is it they say about stats again?
Maybe . . . just maybe . . . tis not that simple.
Maybe . . . just maybe . . . there is a bit more to dr. wilk’s observation.
Maybe . . . just maybe . . . tis not just the poor brown people turning more and more to the ER, scalpel.
I wish they taught stats in medschool . . .
I don’t inquire about the immigration status of my patients. But an increase from 20 to 23% doesn’t seem as impressive as the absolute rate of 80-89%. The insured population is going to have to increase their ER usage drastically to even come close to the overuse of the freeloaders.
As I have said before, and yes it is anecdotal:
If three or more patients from the same family are signing in together to be seen in the ER, it is almost certain that they are covered under Medicaid (and thus they have no copay). Even insured families in car accidents don’t typically check the asymptomatic kids in to be evaluated.
Because it costs them something.
Scalpel: “I don’t inquire about the immigration status of my patients.”
So you just like to make broad (admittedly anecdotal) generalizations about latinos in general, regardless of their immigration status?
How very progressive of you . . . you look beyond residency and stereotype them solely on their brownness.
I hope they realize how lucky they are.
As for the stats, let’s add one more absolute:
Number of visits (in thousands):
Private insurance
2004: 39,344
2005: 45,999
Increase: 6,655
Medicaid/SCHIP
2004: 24,489
2005: 28,661
Increase: 4,172
Regardless of what seems impressive to you, using any of these overly simplistic stats to support such a broad conclusion (“If you subsidize something, you get more of it.”) is either intellectually dishonest or dis-intellectually honest (sincere stupidity). And if you wanted to draw any conclusion about the effects of payment method not muddied by the underlying differences between the populations and you were limited to just this one in-apt measure, you would compare utilization within these distinct groups over time rather than comparing utilization across groups in one year . . .
Unless of course you just want a pretty graph to throw out in support of your pre-conceived and idiotically simplistic conclusion about a very complex and serious issue.
89% is pretty much what I see on that graph. Thanks for the trip down statistical relativity (relative rates of change) but it doesn’t change the actual fact:
89% of those covered by free healthcare used it, in the ED.
Is everyone using the ED more? Yes, clearly. But it’s tremendously illuminating when 89% of those covered in handout healthcare use the ED. (There seems to be a lot of denial underlying the heat of the backlash, a ‘don’t look at the actual problem, what about this’ defense, if you want to get into intellectual dishonesty).
I stand by my conclusion. And I cannot wait until helathcare is free for everyone.
What’s really impressive to me is how consistently “progressives” tend to overvalue their own intelligence compared to those who disagree with them.
Insured families don’t tend to bring the whole clan into the ER for trivial complaints. Those on Medicaid do. Actually, those with low-copay HMOs do the same thing, but the association is not as strong. If you’d ever worked in an ER you’d know that.
Dave’s point is well-taken in that lack of accessibility is probably an issue, but who is to say that any proposed single-payer system is going to provide better accessibility? If reimbursement is poor, primary docs will just refuse to accept that too. And as long as EMTALA is still in force, such people will still come to the ER.
You are certainly entitled to your conclusion and certainly entitled to “pretty much see” only that which you thinks support your conclusion (even if it doesn’t speak to it at all).
What I see is that this statement – “89% is pretty much what I see on that graph” – pretty much explains all one needs to know about your understanding of the “actual problem” (which I pretty much see to be so much more complex and multi-variabled than this term suggests you really grasp).
What I don’t pretty much see is how you can account for the fact that even when you don’t subsidize something (to use your own inartful term), you still get more of it. You can either address my argumnent on intellectual terms or you can make some petulant, dismissive remark . . . but as long as it stands, your argument cannot be right. It is very simple actually.
For the record: I would rather have the intellectual discussion, as I am actually interested in analyzing and solving our health care “problem” with data and logic rather ideology and anecdote.
Scalpel: “What’s really impressive to me is how consistently “progressives” tend to overvalue their own intelligence compared to those who disagree with them.”
What exactly does this mean?
(a) Other than being utterly disgusted by racial bigotry, I am not what anyone would call a “progressive.” Without going in to detail, I will merely offer this in support: we spend more than enough money on healthcare; the failure in the health care market is one of allocation – not neccessarily one inherent to health care itself (though failing to recognize its unique characteristics and treating it like widgets is one of the most clear causes of our current misallocation); given that we waste a lot of money on ineffective or even harmful care, addressing this market failure at the insurance level is putting the cart before the horse and will just make more waste; without wanting to haggle over the numbers I will just point out that more people die because of medicine (iatrogenic deaths, IOM 50,000-100,000, etc) than die because of lack of coverage/access (18,000 or so is the current est.) and also note that this does not account for lives saved because of medicine.
I don’t quite fit the hippy progressive mode.
(b) To ascribe some weird motive (overvalue?) to those who make arguments that are logically more valid and based on premises more accurate is just plain weak. “Intelligence” in the abstract is not at issue. What is valued – by me, conservatives, etc – is the ability to accurately understand and solve problems. I am not sure how that is overvalued, but if so consider me guilty. If I am making an empirical argument, and I am shown that I am empirically mistaken, I actually “overvalue” that too and would try to adjust my understanding accordingly. This is not junior high. I don’t care if that is what drives you, what don’t project that crap on me.
(c) Now to your points: though they are based anecdote – not data, I agree they are indeed intuitive. But I know it is trite but “the plural of anecdote is not data.” More importantly, “if you ever worked in the ER,” or “you don’t what its like to” or whatever version of this that doctors constantly fall back on is just bloody worthless. For various reasons, this is just a non-starter. But I do agree to the extent that this is backed up by the data. We can dig through there and actually look at the number sin that report and we can see. Any trivial use is just ineffeicient waste. But I could see your argument being the case though, but then we have to look at the conclusions you draw re: payment (or lack thereof). Maybe people on Medicaid don’t have a good relationship with their PCP? Maybe if they had more experience in the health care system they might? To say this is solely a matter of the payment incentive is just incredible on its face. Maybe they are having trouble finding PCPs who will treat them.
(d) I have not endorsed “single-payer” but would like to ask you to clarify what you mean by single-payer: In a “single-payer” national health insurance system (Canada, Denmark, Norway, Sweden, etc.) health insurance is publicly administered but [mostly] privately delivered. Great Britain and Spain have “national health services”, where physicians are most salaried and hospitals, publicly owned and operated. If you think single-payer is scary, you’d love to be salaried, huh?
Hopefully, you will at least acknowledge that the “progressive, single-payer, hippy, Michael Moore” label does not quite fit. I am just getting sick and tired of the BS being spewed forth as the health care debate starts to heat up. I offer my criticsm – not in support of one ideology to attack another – but merely as one who takes offense at idiocy.
If you subsidize something, you get more of it:
I once saw a line-graph of out of wedlock births up against increases in medicaid funding for pregnant women and single mothers. Let’s just say the lines rose quite exponentially together.
Aah, if only I’d “Had stats” I’d see the light, and not point out that 89% of people getting public support visited the ED. Except that they did.
Oh, but wait, I have had stats. A good course, during my Masters’ degree. It doesn’t impair me from reading a graph, or from making an easily (and thus far unrefuted) case for cause and effect. You can wax eloquent all you want, but the evidence is right there before you.
Want to specifically refute the premise? Please do so, but spare me statistical relativity. And ellipses.
Stereotypes are typically based on facts, as painful as it is for some “progressives” to accept. Ignoring things that are obviously true because it doesn’t fit one’s concept of political correctness is the ultimate idiocy.
Hispanics are overrepresented amongst families of five or more.
Asians are overrepresented amongst MIT undergraduates.
Blacks are overrepresented amongst NBA players and Olympic 100-yard sprinters (sorry, no link, you’ll have to take my word for it).
Middle-aged white men are overrepresented amongst serial killers, and Muslims are overrepresented amongst suicide bombers.
Do you know what the most common name for baby boys in Texas is? Jose.
Can you guess what race my best friend is, who was also the best man in my wedding? I’ll give you a couple of hints….he has four kids, and his son’s name starts with a J.
Grunt: it is clear what path you’ve chosen. You haven’t addressed my counter argument – which clearly shows that private insurance also “causes” more people to go the ER – but have rather chosen to stomp your feet “I did too have stats . . . and you use punctuation I don’t like, nah.” Touche.
Scalpel: (1) What are you talking about? You are dancing in quicksand (I can’t believe you pulled out the tried-and-true “yeah, well my bestfriend is black, brown, etc.” . . . oh my). Keep defending your stereotypes all you want, but no one is ignoring them. What does this have to do with anything? What is progressive PC crap? You have some weird strawman characature in your mind, but this bears no relation to the words I am typing. I am not disputing your astute – and obvious – racial observations. I am directly and clearly challenging their relevance to a broader debate. Please address my argument not some weird narrative you have going on in your head. Stop projecting weird motives that bear no relation to the words I use to criticize you. (2) You know who else has large families? Catholics. German, Swedish, and Italian Catholic midwesterners would clearly be over-represented even to this day in the areas I have lived. Some Evangelicals now too are beginning to do the same in the Southern areas I live in now. What does your “theory” have to say about how they will use the ER and/or pay for it? Prob’ly need more info, huh? Prob’ly has something to do with socio-economic status, huh? Do large Mexican families with private insuarnce do the same thing in your area? (3) Look, you made a remark – consistent with your observations and prob’ly consistent with underlying family racial demographics of your area. While it may be true descriptively, it is of little operant value. It is gratuitous and uninformative to the issue at hand.
I agree – wholeheartedly – with your unremarkable obversation: “stereotypes are typically based on facts . . .” This applies to all those stereotypes about doctors, too (I won’t lay them all out here but you know what they are, and most of them aren’t as positive as MIT-type stereotypes either). And you and grunt’s responses so clearly reinforce the most cliched and negative steretypes of them all.
Good luck.
Actually, he’s Mormon. He and little Joshua hate Mexicans.
hehehehhe Scalpel.
Pedantics:
<i>July 27th, 2007 at 2:39 am
Aah, if only I’d “Had stats” I’d see the light, and not point out that 89% of people getting public support visited the ED. </i>
The graph represents number of ED visits per 100 people on Medicaid or SCHIP, not the percent of people on Medicaid who used the ED that year. Of course, you’re still comparing apples to apples.
[ed: she meant Gruntdoc, not Scalpel, as I’m the one responsible for the statement. Mea culpa for the misstatement. Does not, as you point out, change the argument.]
So, Dr. Berg, you have no argument besides the one attempt at relative rates of rise to try and cover up for the 89% Fact. But feel free to continue casting my observation in whatever pejorative terms you wish, without actually coming up with something that would explain the gross disparity.
Hmm, nah, couldn’t be subsidization, i.e., delivering a service of value for free, could it? If the privately insured rate of visits, and the publically subsidized rate were anywhere near equal my argument would have no validity. However, they’re not equal. Not even close.
By the way, a google search for “If you subsidize something, you get more of it” shows the phrase isn’t my creation, and the effect has been seen elsewhere.
For the record, I was intentionally saying ‘hhehehehe’ at Scalpel for “tricking” Morris Berg with the Mexican/Mormon thing (comments #16 and #18). I knew GruntDoc said the misstatement (which is also explained incorrect directly under the graph).
There are so many confounding variables that it is impossible to draw the conclusion that getting government healthcare benefits in and of itself leads to an increase in ER visits.
You’ve drawn a conclusion that isn’t valid to conclude and worse, you’re using this non-sequitur to advance a political agenda.
I’m concerned that facts are getting lost in political arguments.
Fact: Emergency departments across the nation are getting swamped with people coming in who are NOT emergency cases.
Fact: There is a significant population in this nation who uses emergency care as primary care.
Fact: This is much more expensive to administer than clinical care or PCP care.
Fact: A very large portion of those using emergency care as primary care do so because that don’t have the means to pay for primary care.
Fact: A high percentage of those using emergency care as primary care are on government-funded programs to pay for medical care.
These are facts.
Do with them as you wish.
Interpretting that subsidies might be part of the cause of the problem (overworked/improperly utilized ED’s) is NOT automatically a symptom of xenophobia or racism, though.
(Uh, and, last time I checked, statistics was part of the med school curriculum. It’s sure as hell part of my graduate curriculum in Criminal Justice.)
Simple solution in my book… you come to the ER with your “free healthcare” (which I pay for so is it really free?) and you dont have an “Emergency” you pay 10$ co-pay before you get you hands on any kind of prescription or pain meds. I have to pay 20$ to see my doc… so should you. In fact if I go to the ER I pay
50$. Then riding out that ant bite on you foot or the cough you have had for 2 hours wont seem so bad. Harsh? Maybe but I am sick of paying for people who dont really deserve the hand outs our government so graciously gives those who are supposedly in need.
This in the comment thread stuck out to me:
I am actually interested in analyzing and solving our health care “problem” with data and logic rather ideology and anecdote.
Classic example of the notion that “people” problems can be solved by applying “data”. People just don’t fit into those little boxes nearly so neatly as data does.
If you subsidize something, you get more of it:
Oh! Subsidize! I thought you said supersize….
oh, how did i miss this??? the logic of the graph escapes me. it’s so unclear. chaos theory is not figured in and when you spoke of illegal’s using the ER i thought you were talking about the Dutch who are all alcoholic spouse-abusers more closely related to the orangutan than humans.
spoke to one of our vascular surgeons today. the hard-core surgical subspecialties, vascular surgery for example, are only filling 75% of their residency spots. it used to be you had to graduate top in your class and top in your residency class to get a vascular spot. now of that 75% fill rate only 80% are american med school grads. there are plenty of great foreign trained docs, but also a much higher proportion of hacks. america is going to get what it wants, ‘free’ health care worth exactly what free stuff is worth… jack shit. i just hope when i retire i know a few practicing docs who know their anal sphincter from their oleacranon.
cheers
GD,
not sure if you saw this one from my colleague on my site but it dovetails nicely with this graph.
http://docsontheweb.blogspot.com/2007/07/revolution.html
cheers
OMg! I’ve seen people do this! Medicaid mavens wanting the non-sick kid to be seen too! It’s free, why not? And we wonder why healthcare is so expensive? Oy Vey!
This Morris Berg seems like one of those pseudo-intellectual ass holes you find at a dinner party talking about a wine he just read about, but really knows nothing about. Then, in order to make a point he just talks louder and louder until everyone else walks away, at which time he feels like he won the argument. Then he mails his check to the DNC/Elect whatever-liberal-dork (you insert the name) campaign fund, making him feel good about himself, the Earth, and the children.
personally, i am against the children.
personally, i am against the children, peace, and tolerance. i’m a big fan of war and racism as well. and i hate the dutch.
RE: James Wilks MD
You had two patients arrive in the ED. Did you see them in the office prior to sending them to the ER or did they go there directly themselves? I’m just curious because I’m an ER nurse who sees on a daily basis PCP sending their patients to the ER for a complete work up when they know full well they will be an admission. Patient #1: 77-HTN-TIA-CRF-N/V and abdominal pain. Is he an admission? I’m guessing yes. Patient #2: 80ish with CAD, S/P CABG, CHF, decreases LVEF. Is he and admission? I’m guessing yes. Why not bypass the ER and make these patients direct admits and take care of these patients on the floor where they need to be, in comfortable beds instead of makeing them pay for an ER visit, an ER doctor visit, and STAT everything. Come on…. give a patient a chance to have money left over to buy his meds.
I’m not implying that all patients from their PCP should go directly to the floor, there are some that need the ER to stabilize, or worse yet, prepare for surgery or are a full blown STEMI, but generally these are not the cases we see in the ER.
What we see and hear is the PCP calling in and saying, “I want my patient seen now and I can do is look around and see patients in the hall and say to myself, where the hell am I going to put this patient.
Hmmmm…. have I gone off on a tangent? I think I did… Sorry about that.
AMEN TO THAT MY SISTER!!!!!! Couldn’t have said it better myself!
Re: MyOwnWoman
Wow.
“If three or more patients from the same family are signing in together to be seen in the ER, it is almost certain that they are covered under Medicaid (and thus they have no copay). Even insured families in car accidents don’t typically check the asymptomatic kids in to be evaluated.”
Absolutely right!
It’s a long way to go for a commentary on socialized medicine, but I promise it’s in here = )
I had a ‘save’ last year that keeps coming to mind; a 70 pound 89 year old dialysis patient with a history of renal failure, multiple strokes completely aphasic and normally has no voluntary movement, found severely hypoxic by the nurses aid. ‘Full Code’ status. Even though we didnt really want to, we used her dialysis catheter as an emergency access, sedated and paralyzed her, since she was clenching her teeth, intubated her and ultimately brought ETCO2 from 80 to 40 before we arrived at the local ER.
The patient’s family wanted everything possible done to ‘save’ great grandma… because ‘she’s not ready to go yet’, so they treated her pneumonia, now she’s back in the nursing home, with a new trach and new peg tube.
So take this person, who is most likely utterly miserable, unable to move, scratch, communicate, or even turn off the TV; How many medicaid and medicare dollars, do you suppose to takes, to warehouse, feed, water, transport, dialyze thrice a week, and provide medical care?
Would it change the opinion of the family members if they had to care for great grandma themselves? Or pay even part of the tab to keep her like she is? Would any politician have the cajones to be outraged by such a thing? It certainly breaks my heart.
Who cares if or why they go to the ER more? Unless they’ve paid SS for years to cover this sort of thing, then they are getting a free ride and it needs to stop!!
FREE for everyone or FREE For NO ONE!! That’s the way it should be.
I’m sick and tiered of working my ass off so someone else can sit back and get free day care, free health insurance, free food stamps, free gas, free fuel assistance, free college, minority job rights, and the list goes on.
If you took all state aid away from people who are capeable of working (not the elderly who had money taken out of their checks for years to cover this sort of thing)and made it mandatory that they pay their bills and take care of their own kids, I bet you any amount of money that you would see a huge decrease in the amount of unwanted pregnancies, and people would find a way to make ends meet.
Go ahead and give people a free ride and they will more then definitely take it.
Who pays for all of this….ME and the rest of us honest, hard working, citizens!! I want to know when it’s their turn to pay up!! When do I get my free ride (after all I’ve paid my dues already)!!
We need to stop PAYING people to make bad choices and bad decisions. We need to start making them accountable for their own actions!! What are we teaching them by giving them a free ride when they make a bad choice? Hmmmmmmmm I wonder?
I agree with the last comment…when do we stop subsidizing. I am in an urgent care and it is invariably the Medicaid patients who bring in 5 kids at a time, cannot fill out forms, do not have their information with them, and bitch royally about how awful it is that Medicaid does not pay for Tylenol caplets over Tylenol tablets….and they insist that I speak their language.
the system is not going to stand this too much longer without a complete breakdown.
Morris sure seems to have a high opinion of his own thoughts. That’s the most interesting way to spell “characature” I’ve ever seen.