I’m lucky enough to work at a big community hospital with a lot of resources, and we get a decent number of transfers from smaller surrounding hospitals. The ED doc is stuck taking the call from the sending doc, to both make sure we have coverage for the specialty they say they need, and to ward off the occasional inappropriate transfer / transfer that would be much better served going elsewhere*.
Recently I took a call, the synopsis of which was ‘unstable angina but normal enzymes, some Q waves on the EKG, and pain free: need transfer because we don’t have cardiology’. Unstable angina is often managed by non-cardiologists, but I accepted, rationalizing it’d be an easy transfer anyway, and you never know.
You never know, indeed. When the patient arrived, the EKG with the ‘Q waves’ they did looked like this:
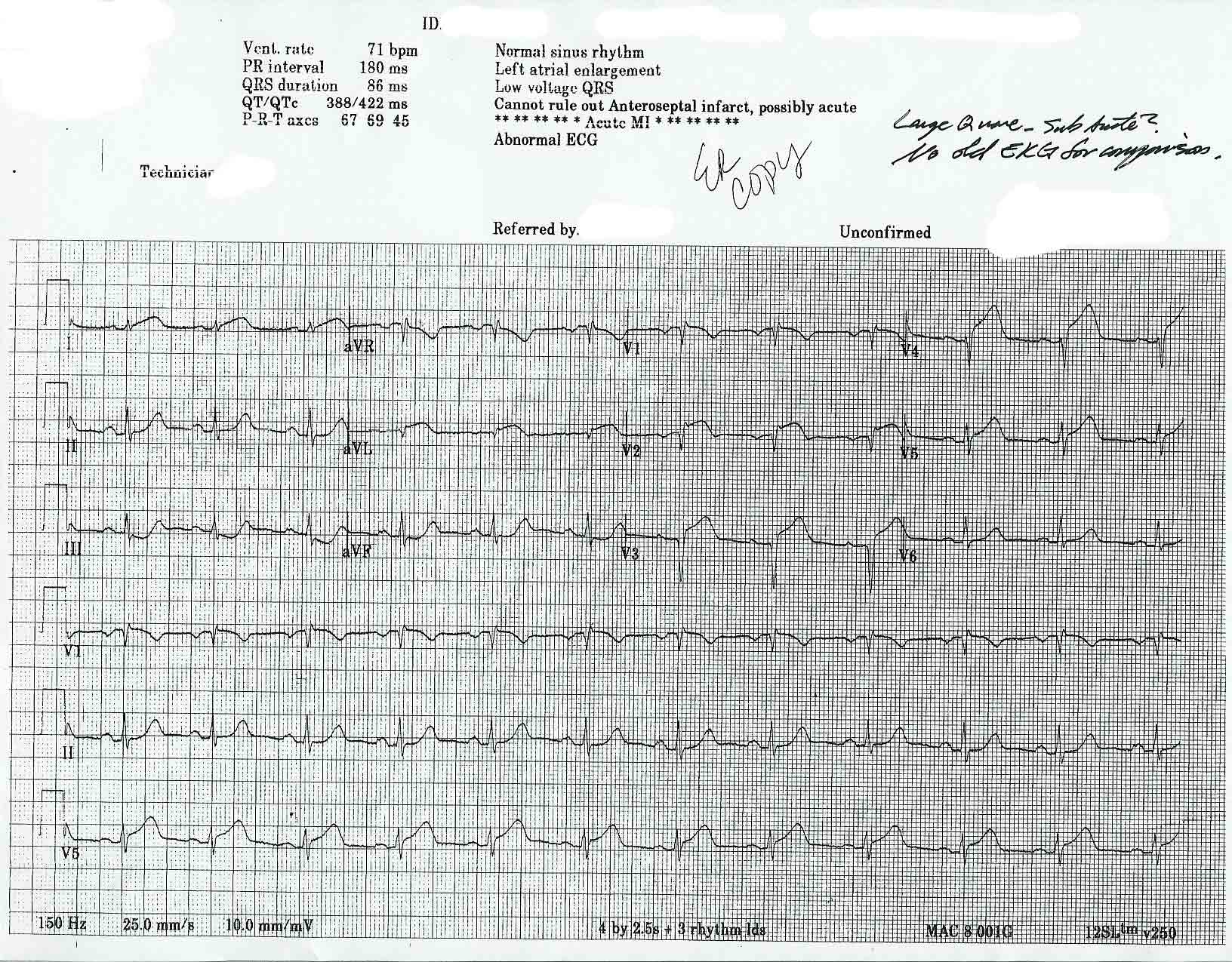
Got a nice quick trip to the cath lab. (For those scratching their heads, this is an acute MI, the machine’s screaming MI in the automated printout, but apparently the doc looking at it didn’t believe it)(the machine is frequently wrong, but you need to look hard at the tracing when it’s saying something you don’t expect).
This will be read as a guy in the Ivory Tower looking down on the little guys in the trenches, and it’s not intended that way. It is why I’m going to accept anything cardiac for a long, long time though…
(* This does not mean I’d commit an EMTALA violation by refusing a transfer, it means sometimes patients are better served elsewhere. For example, while we have a hand surgery call list our joint cannot do re-implantations, so while technically we can handle hand injuries a few patients need transfer to a more appropriate facility).


Hmmm, someone somewhere needs to brush up on their ACLS skills (or to be more fair, EKG interpretation skills) : it would have to smack you in the head to be less obvious.
May need to institute some regular fax EKG reviews on chest pains from that site ? : significant TNK delay if your cath lab was not up and running….
Hey GD… as an MSII, this post made my day. I am finding EKGs very difficult, and thought I had lost complete confidence in my ability to ever make sense of them. Then I read this entry, recognized the pattern on this one quickly, and felt good about myself. Thanks!
We had a similar occurance last year.
Pt was shipped via 2 hr ambulance ride to us for s/p MI. He got cathed, but a bit late though as his troponins peaked at 50!
So much for the 90-minute door-to-balloon time on this one…but hopefully the patient will benefit with their newly-opened artery…
Strong work.
Crap. If by “Q-waves” you mean ST elevations…
I always fold-over the computer interpretation, come up with my own, and then glance back at it to see if I agree or if I’m missing anything, for this very reason. Hmm, why does the computer think this is an Acute MI if I don’t?
Um, I’ve never been officially trained in 12-lead interpretation, and even I can see the ST elevation. Not. Good.
Dear Doc,
Being a patient and having an MI smack dab wired up in the ER in Midland, Tx., is it possible to explain to a layman what you look for?
Rockhead
Midland, Texas
[GruntDoc: having worked there, you’re in good hands. Good luck, and let us know how you do!]
There’s a reason they call them “tombstone T’s”. Showed this to three of our new RN’s, they all got it right and knew the correct treatment. Rest assured GruntDoc that your nursing staff knows what they are looking at when they see elevated ST.
As someone who both accepts transfers from smaller places (ie. remote nursing stations) and also passes along transfers to higher levels of care (the ivory tower a mere jet ride away) I find cases like this most interesting. Certainly it’s a miss, and one with potentially significant consequences. Unfortunately in the medical culture (fear of litigation, perception of feedback as confrontational) of many places there isn’t any way to give the transfering doc feedback, and therefore prevent the error from repeating itself.
My guess is that a fax to the original doc of the ECG, elevated ST segments circled, and a note that says….acute MI, pt. went to the cath lab and did okay…send us a fax of the ECG if you ever want a second opionion…. would probably ingrain that pattern in that particular docs head forever, and probably reduce future errors….
Just some thoughts!
Dr. J.
I don’t see any Q-waves, but I do see some ST-elevation…
Great teaching case for the future–that EKG is totally classic! Love how the computer just says “cannot rule out”, even with hyperacute T-waves and S-T elevation.